HITAP เปิดตัวระบบ THEMS เตรียมยกระดับการบริหารจัดการก๊าซเรือนกระจกของสถานพยาบาลในประเทศไทย
STOCKHOLM — Andemariam Beyene sat by the hospital window, the low Arctic sun on his face, and talked about the time he thought he would die.
Two and a half years ago doctors in Iceland, where Mr. Beyene was studying to be an engineer, discovered a golf-ball-size tumor growing into his windpipe. Despite surgery and radiation, it kept growing. In the spring of 2011, when Mr. Beyene came to Sweden to see another doctor, he was practically out of options. “I was almost dead,” he said. “There was suffering. A lot of suffering.”
But the doctor, Paolo Macchiarini, at the Karolinska Institute here, had a radical idea. He wanted to make Mr. Beyene a new windpipe, out of plastic and his own cells.
Implanting such a “bioartificial” organ would be a first-of-its-kind procedure for the field of regenerative medicine, which for decades has been promising a future of ready-made replacement organs — livers, kidneys, even hearts — built in the laboratory.
For the most part that future has remained a science-fiction fantasy. Now, however, researchers like Dr. Macchiarini are building organs with a different approach, using the body’s cells and letting the body itself do most of the work.
“The human body is so beautiful, I’m convinced we must use it in the most proper way,” said Dr. Macchiarini, a surgeon who runs a laboratory that is a leader in the field, also called tissue engineering.
So far, only a few organs have been made and transplanted, and they are relatively simple, hollow ones — like bladders and Mr. Beyene’s windpipe, which was implanted in June 2011. But scientists around the world are using similar techniques with the goal of building more complex organs. At Wake Forest University in North Carolina, for example, where the bladders were developed, researchers are working on kidneys, livers and more. Labs in China and the Netherlands are among many working on blood vessels.
The work of these new body builders is far different from the efforts that produced artificial hearts decades ago. Those devices, which are still used temporarily by some patients awaiting transplants, are sophisticated machines, but in the end they are only that: machines.
Tissue engineers aim to produce something that is more human. They want to make organs with the cells, blood vessels and nerves to become a living, functioning part of the body. Some, like Dr. Macchiarini, want to go even further — to harness the body’s repair mechanisms so that it can remake a damaged organ on its own.
Researchers are making use of advances in knowledge of stem cells, basic cells that can be transformed into types that are specific to tissues like liver or lung. They are learning more about what they call scaffolds, compounds that act like mortar to hold cells in their proper place and that also play a major role in how cells are recruited for tissue repair.
Tissue engineers caution that the work they are doing is experimental and costly, and that the creation of complex organs is still a long way off. But they are increasingly optimistic about the possibilities.
“Over 27 years, I’ve become more convinced that this is doable,” said Dr. Joseph P. Vacanti, a director of the Laboratory for Tissue Engineering and Organ Fabrication at Massachusetts General Hospital and a pioneer in the field.
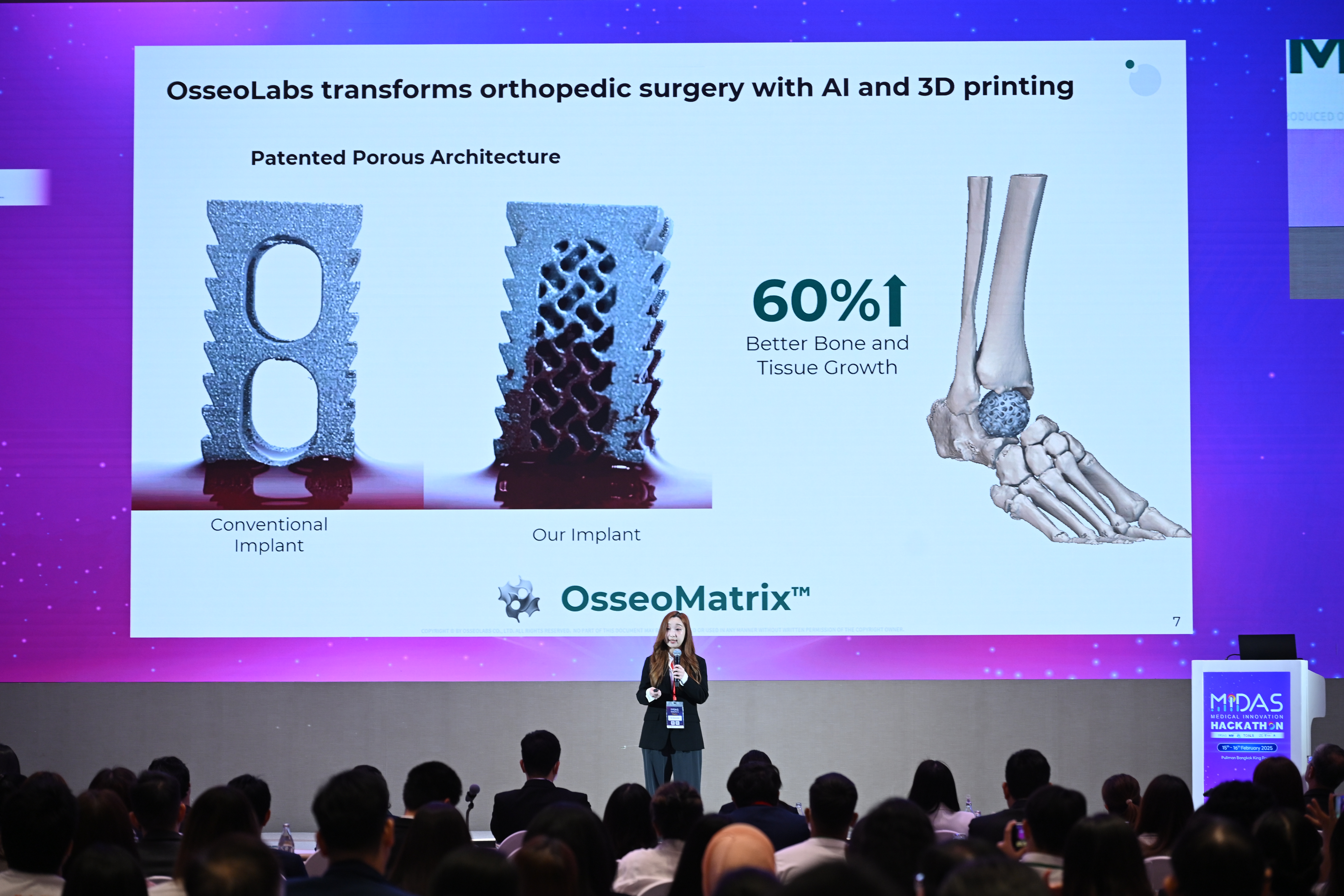
In Mr. Beyene’s case, an exact copy of his windpipe was made from a porous, fibrous plastic, which was then seeded with stem cells harvested from his bone marrow. After just a day and a half in a bioreactor — a kind of incubator in which the windpipe was spun, rotisserie-style, in a nutrient solution — the implant was stitched into Mr. Beyene, replacing his cancerous windpipe.
It was such a seemingly wild scheme that Mr. Beyene had his doubts when Dr. Macchiarini first proposed it.
“I told him, I prefer to live three years and then die,” he said. “I almost refused. It had only been done in pigs. But he convinced me in a very scientific way.”
Now, 15 months after the operation, Mr. Beyene, 39, who is from Eritrea, is tumor-free and breathing normally. He is back in Iceland with his wife and two small children, including a 1-year-old boy whom he had thought he would never get to know. In Stockholm earlier this year for a follow-up visit, he showed the long vertical scar on his chest and spoke quietly in English, the raspiness of his voice a leftover from radiation therapy.
His strength was improving every day, he said, and he could even run a little.
“Things are good,” Mr. Beyene said. “Life is much better.”
Imitating Nature
To make an organ, it helps to know how nature does it.
That is why Philipp Jungebluth, a researcher in Dr. Macchiarini’s lab, had mounted a heart and a pair of lungs inside a glass jar on a workbench and connected them by tubing to another jar containing a detergent-like liquid. The organs, fresh from a sacrificed rat, had slowly turned pale as the detergent dripped through and out of them, carrying away their living cells. After three days the cells were gone, leaving a glistening mass that retained the basic shape of the organs.
These were the heart and lungs’ natural scaffolds, or extracellular matrix — intricate three-dimensional webs of fibrous proteins and other compounds that keep the various kinds of cells in their proper positions and help them communicate.
Labs around the world are now experimenting with scaffolds. In some cases the goal is to use the natural scaffolds themselves to build new organs — to take a donor lung, for example, strip all its cells and reseed it with a patient’s own cells. Why not use what nature has perfected, this line of thinking goes, rather than try to replicate it in a synthetic scaffold?
Dr. Macchiarini and his team tried this beginning in 2008, successfully implanting reseeded windpipes from cadavers in about a dozen patients, most of whom are now living normal lives. Because the donor’s own cells are removed, this approach all but eliminates a major problem of transplants: the risk that foreign tissue will be rejected by the recipient. But it does not solve several other problems that may be just as troublesome. A donated windpipe may not be the right size; it has to be stripped of its cells and reseeded while the recipient waits; and the procedure still requires donor organs, which are in short supply.
So for Mr. Beyene, the decision was made to produce a scaffold out of plastic. But all the work with natural windpipes proved useful. “We learned so much, starting from zero,” Dr. Macchiarini said. “We could have never done the artificial transplant without the past experience.”
Made to Order
Mr. Beyene’s synthetic scaffold was fabricated by scientists at University College London, using scans of his natural windpipe as a template. It was an exquisite piece of polymer engineering, tailor-made to fit his chest.
But it was still just a lifeless piece of porous plastic. To become a working organ, the tiny spaces in the plastic needed to be filled with cells that would eventually function together as tissue. Not just any cells would do; Dr. Macchiarini and his team would start with stem cells.
To ensure that the organ would not be rejected, the cells had to come from Mr. Beyene himself, which also bypasses the kind of ethical issues that have arisen over the use of embryonic stem cells. Mr. Beyene’s stem cells were obtained from his bone marrow. The cells were placed in nutrient solution and then dripped by pipette over the scaffold. It was like basting a turkey.
Human stem cells are part of the body’s system for building and repairing itself. They begin as a blank slate, but are able to become specialized cells specific to particular tissues or organs like the windpipe. In recent years, scientists have made great advances in understanding how stem cells can differentiate in this way.
The Stockholm team was hoping that with the help of stem-cell-stimulating drugs, the marrow cells placed on the windpipe would start to become the right kinds of cells on both the inside and outside of the organ. But Dr. Macchiarini does not think the process worked quite as planned. “I’m convinced that the cells we are putting in the bioreactor after two or three days are gone,” he said. But as they die they release chemicals that signal the body to send more stem cells from the bone marrow through the bloodstream to the site, aiding the regenerative process.
Or at least that is what Dr. Macchiarini thinks happened. “We are far away from understanding this process,” he said. “Far, far away.”
‘If It Bleeds, It Lives’
If you cannot cough, you’re dead.
That sums up one of the important functions of the windpipe: keeping bacteria and other particles in the air out of the lungs, where they could cause potentially fatal infections. A normal windpipe is lined with specialized cells, including some that produce mucus that can trap the particles. Coughing then brings the mucus up and out.
So one test of a tissue-engineered windpipe is whether it contains these specialized cells. In Dr. Macchiarini’s earlier work involving donor windpipes, he had seeded the inside with similar cells taken from the recipient’s nose. But with Mr. Beyene, Dr. Macchiarini was counting on stem cells to differentiate into these other kinds of cells, generating a lining for the windpipe.
In November, five months after the surgery, Mr. Beyene’s windpipe was found to be partly lined with the specialized cells. And in the later follow-up visit, Dr. Macchiarini noted that the lining was still thriving, with no sign of infection. “And he is able to cough,” Dr. Macchiarini said.
If the cells are surviving, that means the windpipe is developing a complex network of tiny blood vessels through the same regenerative process that produced the specialized cells. All tissues must have such a network so that every cell can get oxygen and nutrients. But developing one — or ensuring that one develops — is an enormous challenge for tissue engineers.
“From the beginning, our view was that the principal barrier to this was going to be the blood supply,” said Dr. Vacanti, whose laboratory has long worked on developing a tissue-engineered liver, among other organs.
Mr. Beyene’s doctors had one way to be certain that his windpipe was developing a blood vessel network. As part of their follow-up exam, they purposely injured the internal lining slightly.
“If it bleeds, it lives,” Dr. Macchiarini said.
Mr. Beyene’s windpipe bled.
A Quest Continues
Mr. Beyene hopes to return someday to Eritrea and work as a geothermal engineer. But for now he remains in Iceland, to be close to Stockholm for regular follow-up visits.
The windpipe contains only his own cells, so he does not need to take drugs to suppress his immune system to ward off rejection. But the synthetic scaffold, like any foreign material, caused the body to produce scar tissue, which had to be removed. While that is no longer a problem, Mr. Beyene does not know when, or if, he will be able to return home. “They have to say, ‘Things are perfect; you don’t need any more care,’ ” he said.
“Nobody knows. This is the first case.”
Last November, five months after Mr. Beyene’s surgery, Dr. Macchiarini implanted a bioartificial windpipe in another cancer patient, Christopher Lyles. He used an improved plastic scaffold, made up of even smaller fibers for the cells to be embedded in. Mr. Lyles returned home to Maryland in January but died in March. The family did not release the cause of death, but Dr. Macchiarini said that the implant had been functioning well.
Despite that setback, in June Dr. Macchiarini performed similar operations on two patients in Russia. Both have been discharged from the hospital and are doing well, he said.
Dr. Macchiarini is planning even more operations. But there needs to be a less complex and cumbersome solution, he said, beyond procedures that can cost up to half a million dollars.
Because the need for this kind of work is potentially so enormous, “we cannot pretend that we can reseed with the specific cells outside the body,” he said. Instead, he envisions developing even better scaffolds and implanting them without cells, relying on drugs to stimulate the body to send cells to the site.
His ultimate dream is to eliminate even the synthetic scaffold. Instead, drugs would enable the body to rebuild its own scaffold.
“Don’t touch the patient,” Dr. Macchiarini said. “Just use his body to recreate his own organ. It would be fantastic.”
Monday: Using animal scaffolding to get human tissue growing.

มูลนิธิเพื่อการประเมินเทคโนโลยีและนโยบายด้านสุขภาพ
สำนักงานใหญ่ : 88/22 หมู่ที่ 4 อาคาร 6 ชั้น 6 กรมอนามัย กระทรวงสาธารณสุข ถนนติวานนท์ ตำบลตลาดขวัญ อำเภอเมืองนนทบุรี จังหวัดนนทบุรี 11000
โทร : +662-590-4549
โทรสาร : +662-590-4369
E-mail : [email protected]